An 8-year-old neutered male dachshund was presented to the emergency department for evaluation of respiratory distress. The dog was previously diagnosed with a heartworm disease and was currently undergoing treatment with a “slow kill” method. Physical examination revealed tachycardia at 160/min, right-sided pulmonary crackles, and tachypnea with increased respiratory effort. The point-of-care blood work showed hyperlactatemia at 4.5 mmol/L, PCV/TS of 53%/7.8 g/dl, mild metabolic acidosis, normal electrolytes and renal values. The arterial blood pressure (Doppler) was at 130 mm Hg.
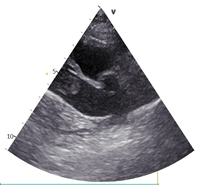
As the dog was getting flow-by oxygen, an abbreviated thoracic point-of-care ultrasound (T-POCUS) was performed (see below).
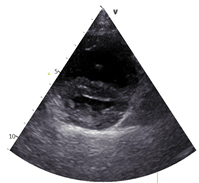
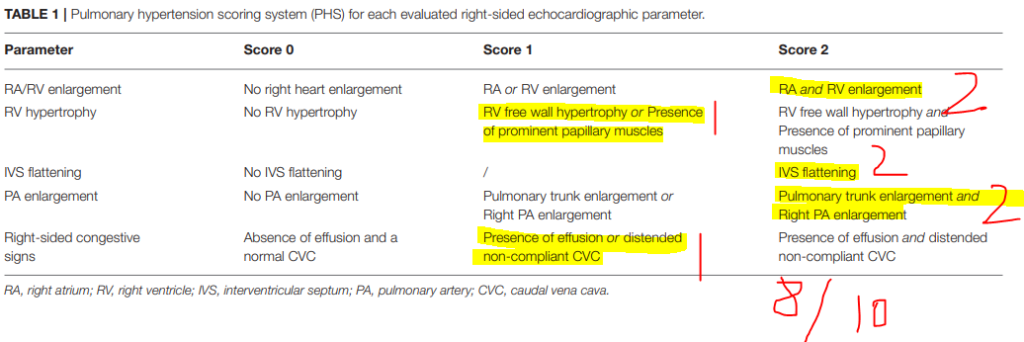
During T-POCUS, the pulmonary hypertension score (PHS, Lyssens et al. Front Vet Sci 2022; table 1) was calculated: 8 out of 10 (77% sensitive and 100% specific for pulmonary hypertension).
Soon after presentation, the dog received a dose of butorphanol 0.2 mg/kg IV and was started on nasal oxygen at 100 ml/kg/min, however his severe respiratory distress persisted, and the decision was made to initiate high flow oxygen therapy (HFOT) with the flow rate 1-2 L/kg/min that resulted in improved respiratory effort and rate. Due to the patient’s respiratory instability, thoracic radiographs were not performed.
The following differential diagnoses were considered based on the combination of the heartworm positive state, suspected severe pulmonary hypertension and unilateral interstitial pattern on the lung ultrasound:
- Pulmonary thromboembolism
- Heartworm disease-induced pneumonitis
- Pulmonary hemorrhage
- PH-induced pulmonary alveolar infiltrates (Kellihan J Vet Card 2015)
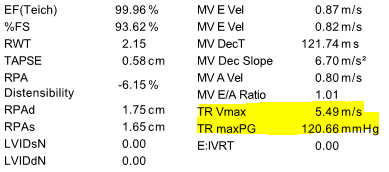
It was decided to perform abbreviated echocardiography in a sternal position to minimize respiratory distress as well as viscoelastic testing, CBC and chemistry. The echocardiogram revealed the following results:
CBC and the chemistry panel came back within normal limits.
The patient was continued on HFOT (1.5 L/kg/min, FiO2=1, T=37C) and received pimobendan (0.25 mg/kg q12h) as well as sildenafil (3 mg/kg q8h) to address right ventricular dysfunction and severe pulmonary hypertension.
Now, let’s pause for a second and consider the following clinical questions:
- Would you consider thrombolytic therapy in this patient?
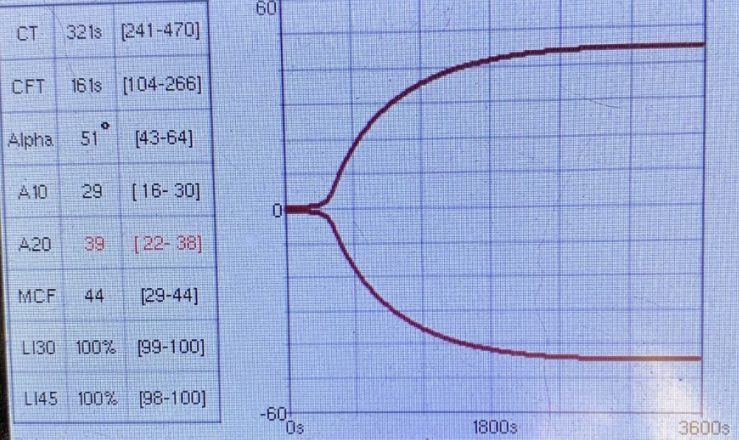
- Why does VCM-Vet results look normal despite the fact that there is a confirmed clot? Should it be hypercoagulable?
- What antithrombotic agent(s) would you consider?
Question 1: Would you consider thrombolytic therapy in this patient?
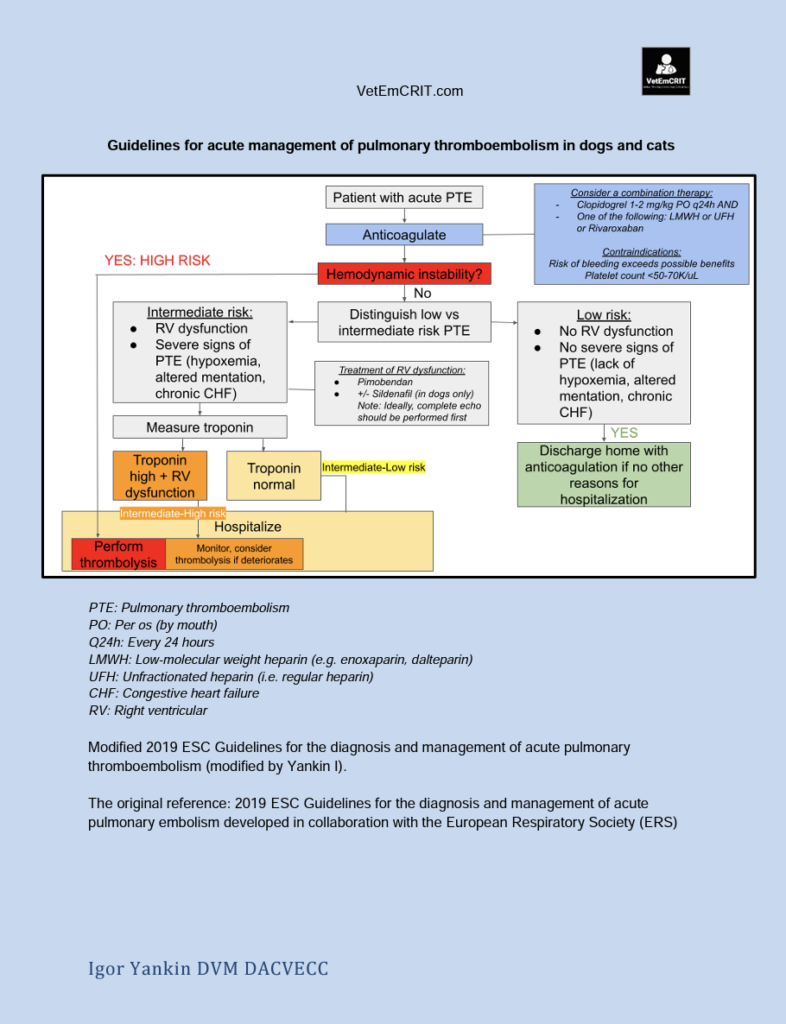
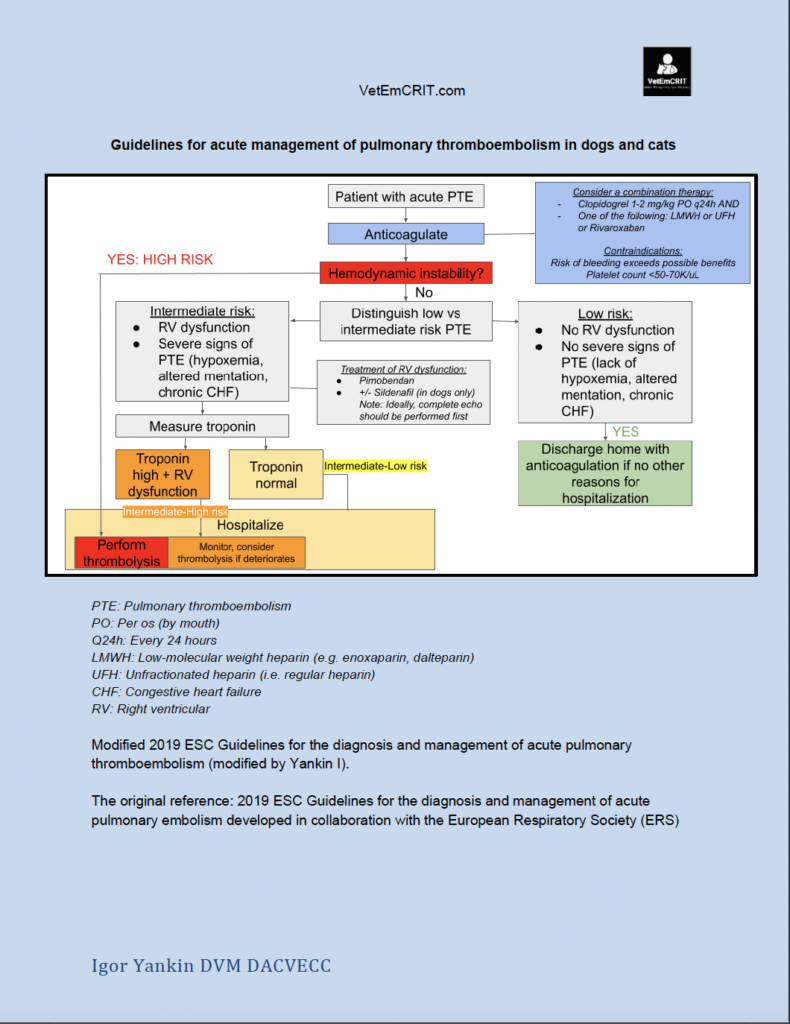
Unfortunately, there is a lack of evidence in veterinary medicine to make any specific recommendations with regard to administration of thrombolytic agents (e.g. tissue Plasminogen Activator, tPA) in dogs and cats with confirmed acute PTE. Therefore, our decision-making was based on human guidelines modified for veterinary medicine (see Figure 5).
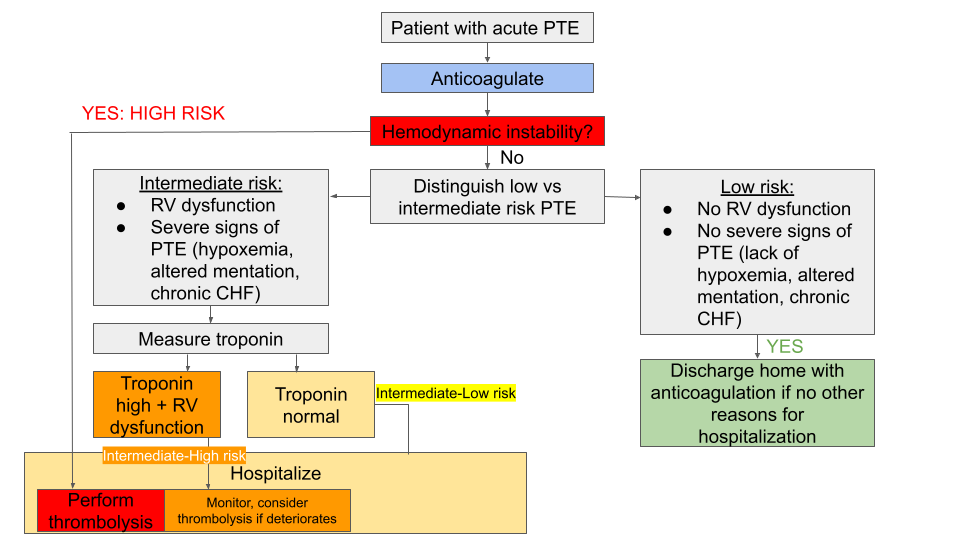
According to the flow chart depicted in Figure 5, our patient was considered an intermediate risk (hemodynamically stable + RV dysfunction + hypoxemia), however the troponin level was not measured. Based on that, it was decided to continue the medical management outlined above (oxygen, pimobendan, sildenafil) + anticoagulation without thrombolysis since he remained hemodynamically stable.
Question 2. Why does VCM-Vet results look normal despite the fact that there is a confirmed clot? Should it be hypercoagulable?
As you may remember, the Virchow’s triad is a series of 3 changes that happen inside the vessels, which determines the formation of venous or arterial thrombus: abnormalities in blood flow (stasis), hypercoagulability, and endothelial damage. Presence of even one or two of these factors may trigger the clotting cascade. Therefore, your patient doesn’t have to be hypercoagulable to form pathologic clots. Our canine patient has been diagnosed with a heartworm disease that by itself may lead to both disruption of the endothelial lining and blood stasis caused by adult worms present in the pulmonary vessels.
The second possible explanation for the absence of hypercoagulability as determined by VCM-Vet is the fact that VCM-Vet is not a perfect test. According to Buriko et al. (Vet Clin Path 2023), the sensitivity of VCM-Vet to identify hypercoagulable patients was poor at 17–33%, while the specificity was excellent at 100%, with TEG set as a reference standard for the purposes of the study. The negative predictive value (NPV) was 87-100%. Since our patient’s VCM-Vet came back as negative for hypercoagulability, there is a 87-100% probability that this negative result was true negative (remember that NPV is the probability that animals with a negative screening test result indeed do not have the condition of interest).
Question 3: What antithrombotic agent(s) would you consider in this dog?
According to the CURATIVE guidelines (Domain 2, Goggs et al. 2019), it is suggested that combination therapy (platelet inhibitor + anticoagulant) may be considered where there is a high risk of thrombosis and the risk of clot formation is felt to outweigh the increased risk of bleeding resulting from combination therapy. Therefore, it was decided to start our canine patient on clopidogrel + a low molecular weight heparin (enoxaparin).
Now, let’s go back to our patient…
The initial therapy resulted in significant improvement of the respiratory status, which allowed clinicians to wean him off HFOT and transition him to 30% oxygen supplementation. His appetite improved as well. However, he suddenly went into a cardiac arrest on day 4 of hospitalization. The necropsy revealed bilateral pulmonary arterial thromboembolism and severe ventricular hypertrophy.
The Bottom Line
- Acute thromboembolism should be suspected in heartworm positive patients presenting with acute respiratory distress.
- Calculation of the pulmonary hypertension score by non-cardiologist clinicians during thoracic point-of-care ultrasound may increase or decrease index of suspicion for pulmonary hypertension.
- Although there is a lack of evidence with regards to management of acute PTE in dogs and cats, stratification of patients with confirmed or suspected PTE into low, intermediate or high risk groups (Figure 5) may help veterinarians to decide whether thrombolytic therapy should be considered or not.
You can download the modified guidelines for management of acute PTE here:
References
- Lyssens A, Lekane M, Gommeren K, Merveille AC. Focused Cardiac Ultrasound to Detect Pre-capillary Pulmonary Hypertension. Front Vet Sci. 2022 Mar 1;9:830275. doi: 10.3389/fvets.2022.830275. PMID: 35300218; PMCID: PMC8920985.
- Kellihan HB, Waller KR, Pinkos A, Steinberg H, Bates ML. Acute resolution of pulmonary alveolar infiltrates in 10 dogs with pulmonary hypertension treated with sildenafil citrate: 2005-2014. J Vet Cardiol. 2015 Sep;17(3):182-91. doi: 10.1016/j.jvc.2015.04.002. Epub 2015 Aug 17. PMID: 26293206.
- Konstantinides SV, Meyer G. The 2019 ESC Guidelines on the Diagnosis and Management of Acute Pulmonary Embolism. Eur Heart J. 2019 Nov 1;40(42):3453-3455. doi: 10.1093/eurheartj/ehz726. PMID: 31697840.
- Goggs R, Bacek L, Bianco D, Koenigshof A, Li RHL. Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE): Domain 2-Defining rational therapeutic usage. J Vet Emerg Crit Care (San Antonio). 2019 Jan;29(1):49-59. doi: 10.1111/vec.12791. PMID: 30654415.
One thought on “Pulmonary thromboembolism in dogs and cats: to lyse or not to lyse? ”