
Stress-free examination of a dyspneic patient is key. A lot of information can be gathered just from observing a dyspneic animal. Assessment of the movement of the chest and abdominal wall relative to one another alongside breathing rate and effort can help refine your differentials and streamline your emergency diagnostics and emergency management.
Commonly used terms to describe abnormal breathing patterns include:
- Asynchronous
- Inverse
- Paradoxical breathing patterns (Sigrist, et al 2011)
These breathing patterns have been shown to have a clinical utility in respiratory localization to the pleural space. Three large scale studies of over 150 dogs and cats found asynchronous breathing, paradoxical breathing or inverse breathing pattern to associated with pleural space disease. They demonstrated these breathing patterns to be highly sensitive for a diagnosis of pleural space disease; i.e animals without pleural space disease are less likely to have paradoxical/asynchronous/inverse breathing than those animals with pleural space disease, but these breathing patterns are less specific for diagnosis of pleural space disease; i.e. by using this breathing pattern alone you are at risk of over-diagnosing pleural space disease (Table 1).
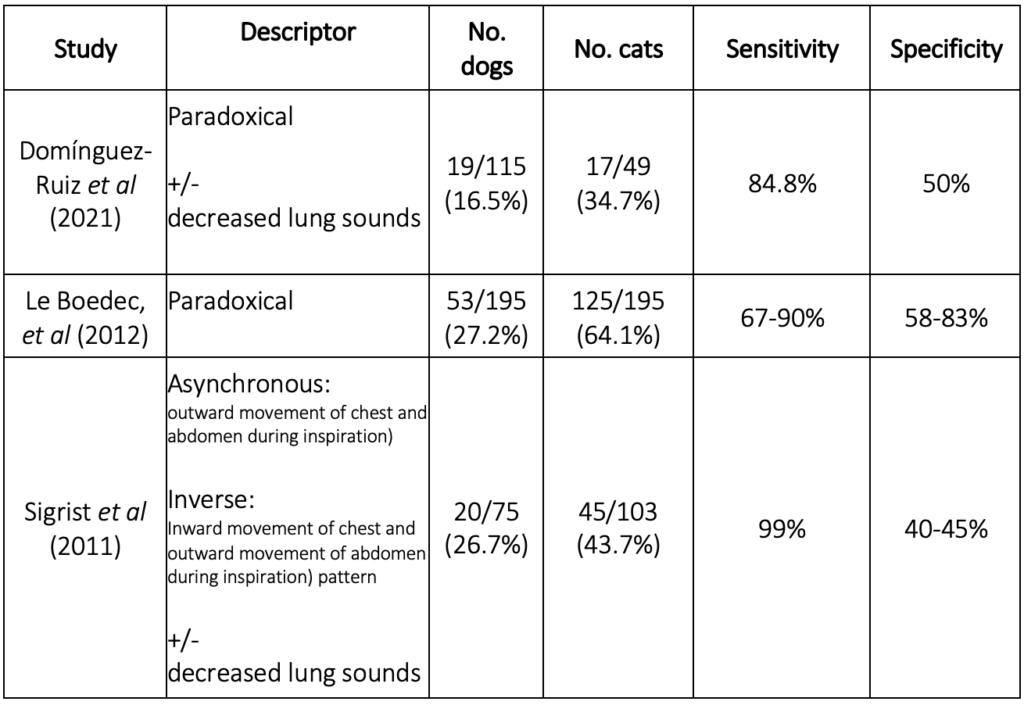
Table 1: Sensitivity and specificity for breathing patterns to diagnose pleural space disease in dogs and cats
Two points of interest are raised from these studies:
1) the physiology behind these breathing patterns
2) the importance and need for using clearly defined terminology
Respiratory mechanics
Firstly, let’s try to understand the physiology that causes pleural space disease to lead to an abnormal breathing pattern. To understand this, we need to understand the normal mechanics of ventilation.
During each breath, air is inspired and moves via the upper and lower airways to the lungs through an active process involving the external intercostal muscles and diaphragm; the external intercostal muscles elevate the ribs and expand the thoracic cavity. The diaphragm contracts and flattens, moving down in the process. The downward movement of the diaphragm further expands the thoracic cavity thereby decreasing pleural pressure, creating a pressure gradient for air flow into the lungs resulting in lung expansion. The downward movement of the diaphragm pushes the abdominal contents down, which forces the abdominal wall out.
Expiration is a passive process – The external intercostal muscles and diaphragm relax, the thoracic wall moves in, and the abdominal wall flatten (Robinson, et al 2002, figure 1A).
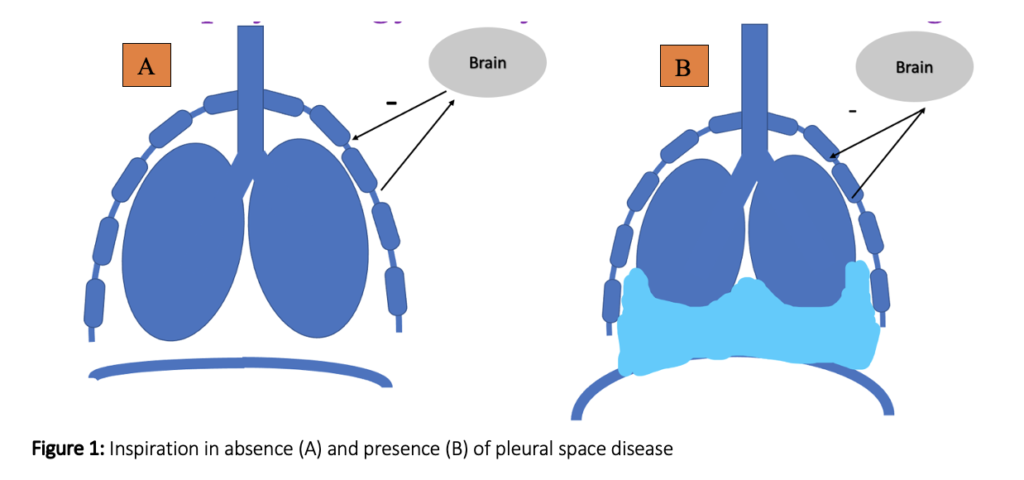
During normal lung expansion pulmonary stretch receptors in the lung are activated and this stretch has a negative feedback effect on external intercostal muscle activity limiting expansion of the thoracic cavity and lung inflation. This is a normal protective mechanism to prevent overdistension of the lungs (Figure 1A).
With pleural space disease (Figure 1B) there is less of a change in pleural space pressure (due to presence of space occupying fluid/viscera) and therefore less pressure gradient for air flow and lung expansion is reduced. This reduces the amount of negative feedback on the external intercostal muscles resulting in prolonged external intercostal muscle activity. This uninhibited expansion of the chest wall, overrides the effect of diaphragm contraction on the abdominal contents and instead pulls the abdominal contents in resulting in a sunken abdomen as the ribs elevate. Giving the appearance of the abdomen moving in as the chest moves out (figure 1B/video 1).
Other diseases found to be associated with these breathing patterns in the aforementioned studies include intra-and extra-thoracic airway disease, chest wall disease, pulmonary and neurological disease. From the schematics you can hopefully appreciate how diaphragm dysfunction (primary or secondary to neurological issue or abdominal pathology) can cause an apparent inward movement of the abdomen during chest wall expansion. If the diaphragm is not able to contract and flatten on inspiration the abdomen doesn’t move outwards and may appear to be sucked as the action of external intercostal muscles continue to expand the chest wall (De Troyer, 1982).
The diaphragm is innervated by the phrenic nerve which exits the spinal cord around cervical vertebrae 4-6. So spinal injury in this region can lead to diaphragm dysfunction – not uncommonly sign with cervical disc disease. Chest wall injury or disease conversely leads to little-no chest wall movement during inspiration and may appear to move in as the outward abdominal movement is more pronounced.
Upper airway obstruction results in a greater flattening of the diaphragm in inspiration as it descends maximally increasing the negative airway pressure to overcome the marked airway resistance. The abdominal contents are pushed down and out and this increased negative pressure, with normal feedback inhibition of the external intercostal muscle activity leads to inward movement of the chest.
In cases of chronic airway obstruction, the ribs are drawn in during inspiration, due to the distorted action of a dysfunctional diaphragm secondary to the presence of lung hyperinflation (Gilmartin, 1986; Troyer, 1985). Both extra- and intra-thoracic airway obstruction lead to inward movement of the chest and outward movement of the abdomen during inspiration, the opposite to that is seen with pleural space disease.
Terminology
In light of the different pathologies associated with these breathing patterns the question is can we refine our differentials by refining our description of the breathing pattern?
Let’s re-consider the medical definitions of the terminology used interchangeably in the veterinary studies; asynchronous, paradoxical, inverse breathing patterns.
In people asynchronous breathing is used to describe the thoracic and abdominal wall moving in opposite directions, paradoxical breathing is defined as the thoracic or abdominal wall moving in during inspiration and moving out during expiration, i.e. paradox to what is normal. Inverse breathing pattern is reserved to describe an inward movement of the chest and outward movement of the abdomen during inspiration.
In people an inverse breathing pattern, inward movement of the thorax has been associated with chest wall injuries secondary to intercostal muscle injuries and/or fractured ribs as well as secondary to intra- and extra-thoracic airway obstruction (Sarkar, et al 2019).
In veterinary patients who can’t be instructed when to breathe in and out it is difficult to determine when inspiration and expiration are occurring, without relying on the chest wall movement. It may be possible to determine inspiration or expiration by watching air movement at the mouth or nares relative to the chest wall movement to better characterize which is moving abnormally; the chest or abdominal wall (video 2).
This may help us refine our differentials alongside other respiratory physical examination parameters such as presence of inspiratory noise, audible wheezes or crackles on auscultation or reduced lung sounds (Domínguez-Ruiz et al 2021, Sigrist, et al 2011).
Often in an emergency it is not possible to refine the differential beyond a difference in chest and abdominal wall movement. Therefore, to avoid confusion it is recommended to just state what you see; the term asynchronous breathing pattern encompasses both abnormal chest and abdominal wall movements and should be applied in this situation.
The Bottom Line
Although many diseases haves been associated with asynchronous breathing patterns, the detection of pleural space disease dramatically alters your diagnostic approach and therefore if you see any patient with asynchronous breathing the first line diagnostics is to rule out pleural space disease. This can be easily done in the emergency room with thoracic point-of-care ultrasound. Future studies with more clearly defined definitions are required to better define breathing pattern terminology to help determine if these breathing patterns can help refine our differentials further.
References
- Domínguez-Ruiz M, Reinero CR, Vientos-Plotts A, Grobman ME, Silverstein D, Gomes E, Le Boedec K. Association between respiratory clinical signs and respiratory localization in dogs and cats with abnormal breathing patterns. Vet J. 2021 Nov;277:105761
- Le Boedec, K., Arnaud, C., Chetboul, V., Trehiou-Sechi, E., Pouchelon, J.L., Gouni, V. and Reynolds, B.S., 2012. Relationship between paradoxical breathing and pleural diseases in dyspneic dogs and cats: 389 cases (2001–2009). Journal of the American Veterinary Medical Association, 240(9), pp.1095-1099
- De Troyer, A.N.D.R.E. and Kelly, S.U.Z.A.N.N.E., 1982. Chest wall mechanics in dogs with acute diaphragm paralysis. Journal of Applied Physiology, 53(2), pp.373-379.
- Gilmartin JJ, Gibson GJ. Mechanisms of paradoxical rib cage motion in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1986;134:683–7.
- Robinson NE. Overview of respiratory function: Ventilation of the lung. In: Cunningham JG, Klein BG, editors. Textbook of Veterinary Physiology. 3rd ed. Philadelphia, Pennsylvania: Saunders; 2002. pp. 468–478
- Sarkar M, Bhardwaz R, Madabhavi I, Modi M. Physical signs in patients with chronic obstructive pulmonary disease. Lung India. 2019 Jan-Feb;36(1):38-47.
- Sigrist, N.E., Adamik, K.N., Doherr, M.G. and Spreng, D.E., 2011. Evaluation of respiratory parameters at presentation as clinical indicators of the respiratory localization in dogs and cats with respiratory distress. Journal of veterinary emergency and critical care, 21(1), pp.13-23
- Troyer AD, Wilson TA. Action of the diaphragm on the rib cage. J Appl Physiol (1985) 2016;121:391–400.