Potassium functions as the primary cation inside cells. More than 95% of the total body potassium resides within the cells. Abnormal serum potassium levels may arise due to disturbances in potassium intake, imbalances in internal potassium distribution, or issues with external potassium excretion.
Changes in how potassium is distributed within cells, such as when ß-adrenergic stimulation (as seen in albuterol toxicosis) prompts the movement of potassium in the liver and muscle cells, are usually temporary. On the other hand, a prolonged lack of potassium intake or excessive potassium loss can lead to sustained hypokalemia.
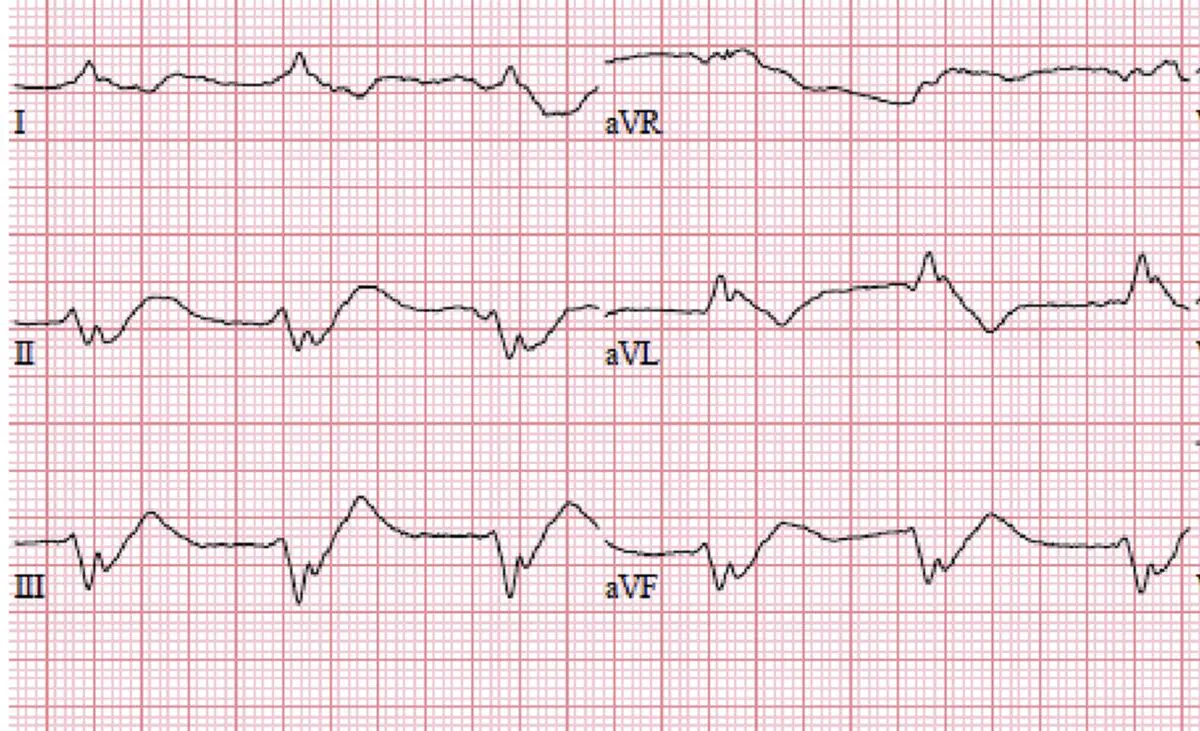
Even though hypokalemia caused by the shift of potassium within cells is temporary, potassium supplementation may be necessary when hypokalemia is moderate to severe, especially if there are observable symptoms like arrhythmia and/or muscle weakness. However, the rate at which potassium is supplemented may need adjustment to prevent a condition called ‘rebound hyperkalemia,’ which can occur after the cause of the potassium shift is resolved.
Continue reading “Avoiding Overcorrection: Rebound Hyperkalemia Awareness”