
An approximately 9-year-old domestic long-haired neutered male cat was presented to his primary veterinarian for evaluation of decreased appetite, possible oral pain, and difficulty chewing food. The cat had previously undergone splenectomy and was diagnosed with a disseminated mast cell tumor that was controlled by palladia and prednisolone.
In the following several days, he was treated with a combination of gabapentin, mirtazapine, buprenorphine, intravenous and subcutaneous fluids for suspected dental pain vs. feline orofacial pain syndrome (FOPS). A couple of days later, the cat developed worsening lethargy, hypersalivation, third eyelid elevation, tachycardia, and arterial hypertension that resulted in hospitalization at his primary veterinarian to continue supportive care. The veterinarian suspected a possible serotonin syndrome induced by a combination of mirtazapine and buprenorphine.
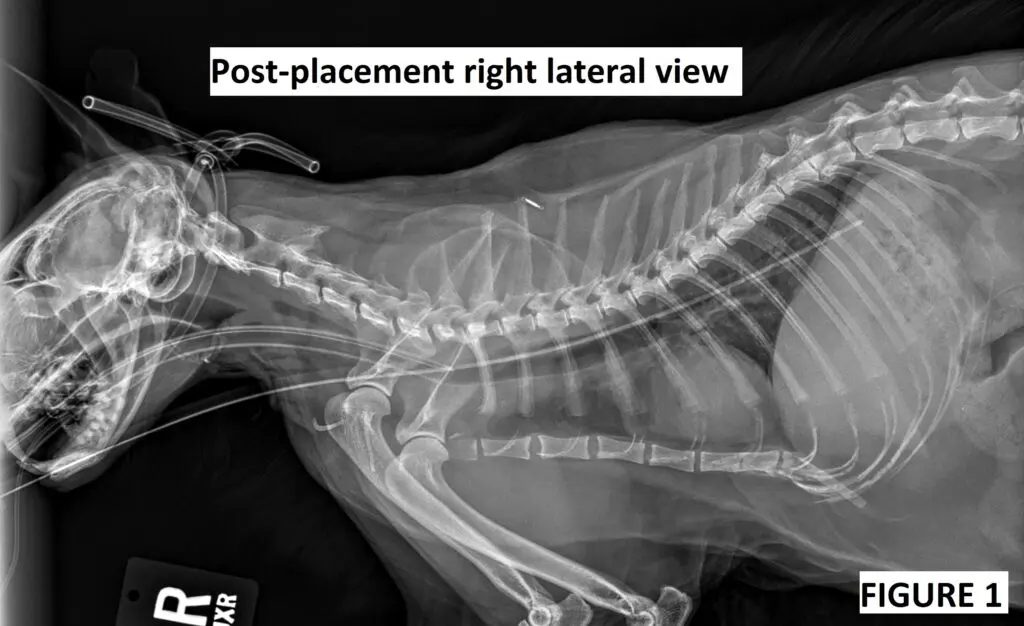
Due to ongoing discomfort while eating and progressively worsening appetite during hospitalization, the veterinarian elected to place an esophagostomy tube under general anesthesia. It was reported that the veterinarian felt some resistance during the tube advancement, but upon reviewing post-placement radiographs (Fig. 1), it was decided that the tube was placed correctly.
During the first feeding, the cat vocalized, and a repeated single lateral radiograph was performed (Fig. 2), which was also interpreted as correct placement. The veterinarian felt more comfortable making this conclusion based on the fact that there was food in the gastric lumen; however, the cat had not been completely anorexic. In the next 24 hours, the cat continued to have mild discomfort during tube feedings, but this discomfort seemed to resolve within short periods of time.

Forty-eight hours after the esophagostomy tube placement, the feline patient rapidly decompensated, manifesting as worsening mentation, hypothermia, increased respiratory rate and effort, as well as cardiovascular instability. Thoracic radiographs were performed (Fig. 3a and 3b).


Figure 3a and 3b. Thoracic radiographs performed 2 days after the esophagostomy tube placement and multiple feedings.
At this point, the primary veterinarian diagnosed pleural effusion, and a diagnostic thoracentesis revealed 14 ml of purulent material with intracellular cocci. An “esophageal tear” was suspected by the primary veterinarian, and a positive contrast study with 2 ml of iohexol diluted in 5 ml of saline was performed (Fig. 4a). The esophagostomy tube was pulled by the veterinarian. Unfortunately, it was elected to humanely euthanize the cat within the next 24 hours due to deteriorating respiratory effort, low body temperature, and worsening mentation.

Case discussion
The first set of recheck radiographs (Fig. 2) obtained immediately after the first feeding was consistent with the mediastinal placement of the esophagostomy tube. This was based on the newly developed pneumomediastinum and pleural fluid, which were not present immediately post-placement several hours prior.
Unfortunately, the misplacement was not recognized at the initial recheck, and the cat continued to be fed through the tube. The radiographs retaken 2 days later showed a significant worsening of pleural effusion and pleural gas, consistent with pyothorax, which likely resulted in septic shock. The distribution of contrast in the last image (Fig 4a) proves that the tube was not in the esophagus, and contrast was leaking into the caudal mediastinum.
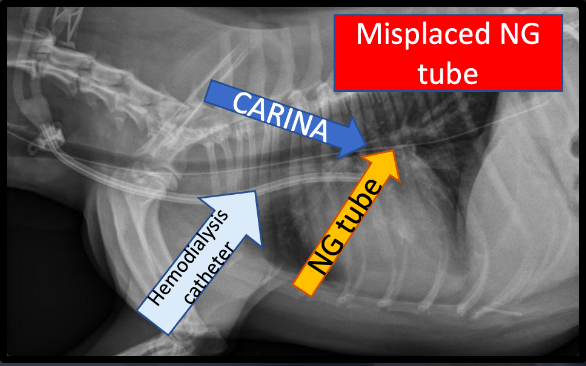
Was it possible to recognize the misplacement on the first set of radiographs taken immediately post-placement (Fig 1)?
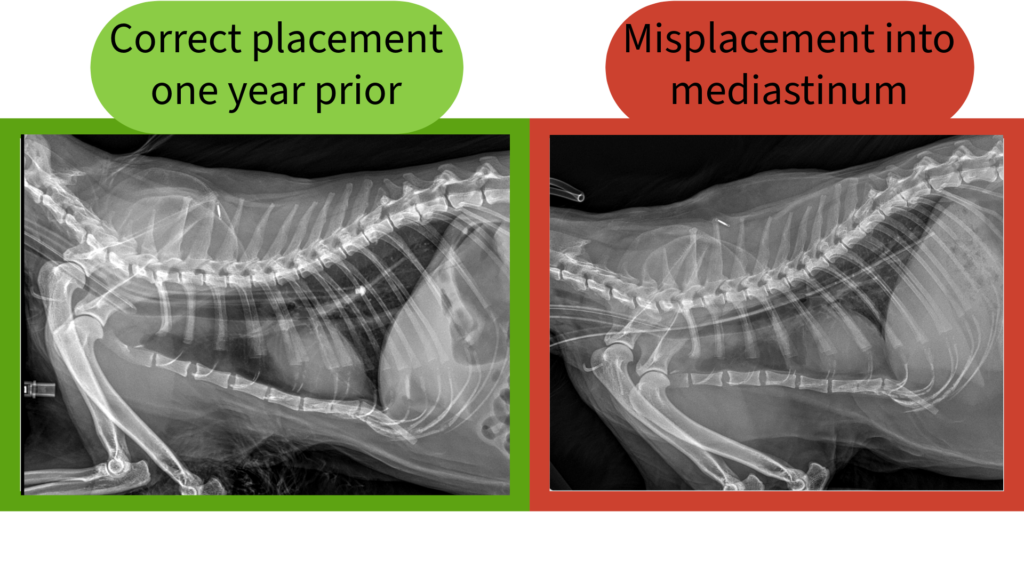
Although the first image taken immediately post-placement looked very suspicious, it is difficult to determine the exact location based on the initial image (Fig. 1). By looking at Figure 5, readers may compare the misplaced tube with the previously correctly placed esophagostomy tube in the same cat one year prior.
In theory, an orthogonal view could have potentially been very helpful but could have also still potentially mimicked correct placement. The definitive confirmation of the esophagostomy tube placement would require the use of positive contrast as it is done in some institutions. It may be especially important in situations when the procedure doesn’t go smoothly and resistance is met during placement of the tube.
How common is the mediastinal misplacement of esophagostomy tubes in dogs and cats?
It is very uncommon. To my knowledge, there is only one case report published by Kelly et al. in the Canadian Veterinary Journal (2022). In that case report, an 8-year-old Siberian forest cat received an esophagostomy tube by her primary veterinarian due to continued anorexia after endoscopic removal of the trichobezoar. The veterinarian placed the tube into the left lateral neck using a standard technique. A single left lateral thoracic radiograph (with radiologist interpretation) showed an endotracheal tube in place and another radiopaque tube superimposed over the neck and thorax, with the exact location of this tube difficult to determine.
Esophagostomy tube feedings were initiated several hours after placement, and the cat was discharged the next day. The cat was returned to the primary care veterinarian the following day for respiratory distress and then transferred to the emergency service. The tube was removed by the veterinarian prior to presentation to the emergency service. At the referral hospital, the cat was diagnosed with pyothorax, and the exploratory thoracotomy was eventually performed that revealed that ‘the area dorsal and left of the trachea was impacted with cat food and blood, an entry wound from the left lateral neck was contiguous with the skin, retropharyngeal hemorrhage and food impaction, extension of food into the cranial mediastinum, and no evidence of any incision ever being made into the esophagus‘ (Kelly CVJ 2022).
The authors discussed that prevention of erroneous mediastinal esophagostomy tube placement could be accomplished by ensuring that the forceps placed into the esophagus are exposed through the skin incision on the left lateral neck when introducing the esophagostomy tube. This would guarantee that the esophagostomy tube enters the esophagus.
The Bottom Line
- The misplacement of the esophagostomy tube into the mediastinum is possible and now has been described in at least two feline patients.
- Placement should always be confirmed with thoracic radiographs, and if the procedure was not straightforward or the position of the tube was uncertain, additional radiographic views, with contrast, should be performed.
- Any discomfort noticed during feeding through the esophagostomy tube should prompt a veterinarian to perform a contrast study to definitively confirm the tube position.
- There is no such thing as a “routine procedure.” Every procedure in veterinary medicine has its own risks that should be respected by attending veterinarians and veterinary technicians.
References
Kelly S, Bandt C. Inadvertent placement of an esophagostomy tube into the mediastinum of a cat. Can Vet J. 2022 Nov;63(11):1124-1128. PMID: 36325406; PMCID: PMC9559027.
This happened to my cat. He died less than 24 hrs after tube placement.