
In animals and humans, phosphorus plays a crucial role in the synthesis of several compounds that are vital for maintaining cellular membrane integrity, energy stores, metabolic processes, and biochemical messenger systems. These compounds include ATP, guanosine triphosphate, cyclic adenosine monophosphate, and phosphocreatine (Yanagawa et al. 1994; DiBartola et al. 2012). Phosphate is a molecular anion that contains phosphorus. Approximately 80-85% of phosphate resides in the bone and teeth as inorganic hydroxyapatite, 14-15% in soft tissues, and less than 1% in the extracellular space (Yanagawa et al. 1994; DiBartola et al. 2012). The body and plasma contain both organic and inorganic phosphates, though blood chemistry analyzers measure only inorganic phosphates.
Bones serve as the body’s phosphate reservoir, offering a readily available source during periods of hypophosphatemia under the regulation of parathyroid hormone (PTH) and calcitonin. Serum concentrations of phosphate, as measured by blood chemistry analyzers, may not accurately reflect whole-body phosphate balance, given that phosphate is the predominant intracellular anion. Similar to potassium, rapid shifts of phosphate between extracellular and intracellular spaces can occur.
Hypophosphatemia can result from:
- Decreased intestinal absorption
- Transcellular shifts (the most common cause): alkalemia, hyperventilation, refeeding syndrome (watch VETEMCRIT video here), parenteral nutrition, insulin administration, glucose administration, catecholamine release or administration, and salicylate toxicity.
- Increased urinary excretion
- Multifactorial etiologies
Degree of hypophosphatemia
- Mild hypophosphatemia (2-2.7 mg/dl OR 0.65-0.9 mmol/L)
- Moderate hypophosphatemia (1-2 mg/dl OR 0.33-0.65 mmol/L)
- Severe hypophosphatemia (<1 mg/dl OR <0.33 mmol/L)
Mild to moderate hypophosphatemia (1-2.7 mg/dl) may not always be clinically significant and is typically asymptomatic.
Severe hypophosphatemia (<1 mg/dl) is generally clinically significant and linked to total body phosphate depletion. This degree of hypophosphatemia and total body phosphate depletion can lead to widespread cellular dysfunction, resulting in consequences such as:
- Hemolysis
- Reversible myocardial dysfunction and cardiac dysrhythmias
- Skeletal muscle changes including rhabdomyolysis
- Neurologic signs such as ataxia, seizures, and coma
- Gastrointestinal signs such as anorexia, nausea, functional ileus, vomiting, and diarrhea
Decision to treat hypophosphatemia
The decision to treat hypophosphatemia depends on factors like the severity of the deficit, suspicion of total body phosphate depletion, anticipated duration of illness, clinical signs, and comorbidities associated with decreased intake or increased loss of phosphate. Parenteral replacement is recommended for patients with severe hypophosphatemia (<1-1.5 mg/dl) at high risk of deleterious sequelae due to phosphate depletion.
Intravenous phosphate administration
The most common intravenous formulation that contains phosphorus is potassium phosphate (K-Phos) available in the USA and some other countries.
In the USA, K-Phos contains the following concentrations of potassium and phosphorus:
- Potassium = 4.4 mEq/ml
- Phosphate = 3 mM/ml (mM/ml = mmol/ml).
If you practice outside of the USA, make sure you know what specific formulation you have available before calculating the administration rate.
It is important to remember that phosphate-containing solutions are INCOMPATIBLE with solutions that contain any calcium salts such as LRS, calcium gluconate, etc.
Potassium phosphate injection is reportedly physically compatible with the following IV solutions: dextrose (any concentration), 0.45% to 0.9% sodium chloride, and sterile water.
As you might know, the VETEMCRIT Excel-based calculator (watch video here) has a tab – “Phosphorus” – that will greatly improve your efficiency when developing a plan for phosphate supplementation.
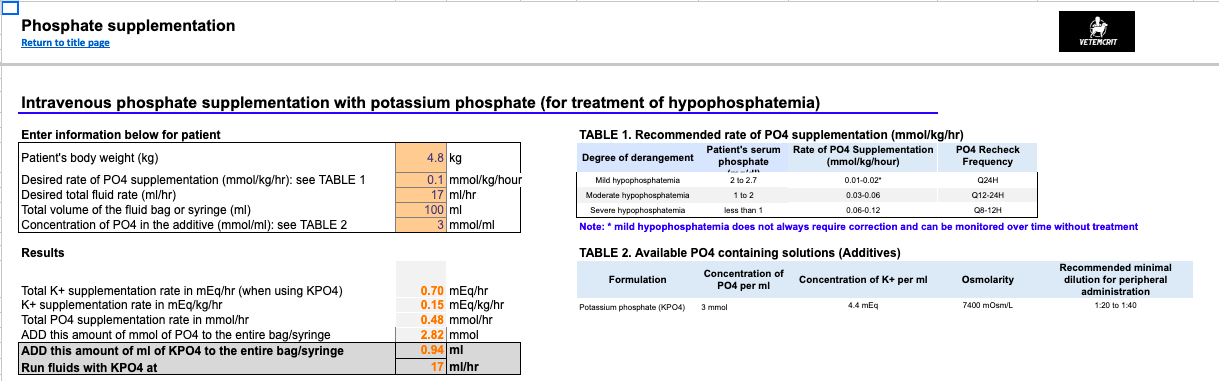
Figure 1. Phosphorus supplementation tab of the VETEMCRIT calculator.
Hypophosphatemia is recommended to be corrected using the following rate: 0.01 to 0.12 mmol/kg/hour. The rate of phosphate supplementation will depend on the degree of hypophosphatemia.
In general, I recommend the following guidelines:
- Mild hypophosphatemia (2-2.7 mg/dl OR 0.65-0.9 mmol/L): 0.01-0.02 mmol/kg/hour of phosphate (recheck q24h)
- Moderate hypophosphatemia (1-2 mg/dl OR 0.33-0.65 mmol/L): 0.03-0.06 mmol/kg/hour (recheck q12-24h)
- Severe hypophosphatemia (<1 mg/dl OR <0.33 mmol/L): 0.06-0.12 mmol/kg/hr (recheck q6-12h)
The step-by-step approach to intravenous phosphate supplementation
Step 1: Choose your phosphate supplementation rate (depending on your preferences and the mentioned-above recommendation; also see Table 1 of Phosphorus tab in the Excel-based calculator).
Step 2: Calculate a total amount of phosphate a patient will need to be supplemented with per hour.
Step 3: Come up with the total fluid rate based on your patient’s needs.
Step 4: Calculate how many hours your bag of fluids will last with the current fluid rate.
Step 5: Calculate how much K-Phos solution you should add to a liter bag.
Step 6: Calculate how much potassium this patient will be receiving with this K-Phos supplementation rate. When using this protocol, it is important to account for all sources of potassium being administered to the patient in the overall fluid therapy plan to minimize the risk for hyperkalemia.
Case example:
A 10-kg spayed female Dachshund with diabetic ketoacidosis (DKA) has serum potassium of 3 mmol/l (reference interval, 3.5-5 mmol/L), serum phosphate of 1 mg/dl (reference Interval, 2.9-6.2 mg/dL OR 0.94-2 mmol/L). She is currently euhydrated and is receiving a fluid rate of 40 ml/hr to account for her maintenance and ongoing losses due to polyuria.
Step 1: Choose your phosphate supplementation rate: you decided to supplement 0.1 mmol/kg/hr of phosphate according to the above guidelines.
Step 2: Calculate a total amount of K-Phos the dog will need to be supplemented with per hour: 10 kg x 0.1 mmol/kg/hr = 1 mmol/hr or 0.33 ml (1 mmol divided by 3 mmol/ml of K-Phos solution = 0.33 ml) per hour.
Step 3: Come up with the total fluid rate based on your patient’s needs: This has already been determined to be 40 ml/hr (will account for maintenance and ongoing losses).
Step 4: Calculate how many hours your 1 L bag of fluids will last with the current fluid rate: 1000 ml : 40 ml/hr = 25 hours
Step 5: Calculate how much K-Phos you should add to a liter bag: 25 hours x 0.33 ml (or 1 mmol) = 8.25 ml (25 mmol) of K-Phos to be added to a one liter of IV fluids to supplement 0.33 ml (1 mmol) of K-Phos per dog per hour.
Step 6: Calculate how much potassium this patient will be receiving with this K-Phos supplementation rate: 0.33 ml/hr of K-Phos x 4.4 mEq/ml of K+ in K-Phos solution = 1.45 mEq/hr = 0.145 mEq/kg/hr of K+ supplementation. Since this dog has a hypokalemia of 3 mmol/l, this amount of K+ may be enough (see Table 1 in the Potassium tab of the VETEMCRIT calculator).
If hypokalemia is more severe (e.g. <3 mmol/L), you may add more KCL to the same bag that already contains K-Phos.
References
Yanagawa N, Nakhoul F, Kurokawa K, et al. “Physiology of phosphorus metabolism.” In Narins RG (editor): Maxwell & Kleeman’s Clinical Disorders of Fluid and Electrolyte Metabolism, 5th edition. New York: McGraw-Hill; 1994.
DiBartola SP, Willard MD. “Disorders of phosphorus: hypophosphatemia and hyperphosphatemia.” In DiBartola SP (editor): Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice, 4th edition. St. Louis: Elsevier Saunders; 2012.
Small Animal Critical Care Medicine, 3rd Edition ; Authors : Deborah Silverstein & Kate Hopper ; Date of Publication: 12/2022
One thought on “Intravenous phosphate supplementation in dogs and cats”