Assessment of the intravascular volume status is a critical skill for emergency veterinarians. Point-of-care ultrasonography (POCUS) is emerging as a valuable, noninvasive, cage-side diagnostic tool for objective evaluation of physiologic and hemodynamic parameters related to volume status, fluid tolerance, and responsiveness. Rapid cage-side sonographic evaluation can obtain qualitative data on cardiac function even when performed by non-cardiologists. POCUS involves answering focused clinical questions using cage-side ultrasonography and increases the sensitivity of the conventional physical examination.
That said, POCUS findings should be interpreted in conjunction with other clinical parameters—such as conventional perfusion parameters (heart rate, mentation, body temperature, mucous membrane color, CRT, pulse quality), urine output, blood pressure, and body weight —and not viewed as an alternative to physical examination or standard imaging studies.
In this blog post, I will describe the most commonly used views to assess volume status in dogs and cats: focused sonographic assessment of the heart (cardiac POCUS) and caudal vena cava (CVC POCUS).
Cardiac POCUS
Cardiac POCUS can be performed in sternal recumbency and/or lateral recumbency. This may depend on operator’s preference and patient’s comfort, presence or absence of respiratory distress, shock and concurrent injuries.
Step 1: Rule out pericardial effusion and sonographic cardiac tamponade.
- Assess pericardial space via subxiphoid and right parasternal view for the presence of pericardial effusion with or without signs of sonographic cardiac tamponade (diagnosed via right atrial +/- right ventricular wall collapse during diastole)
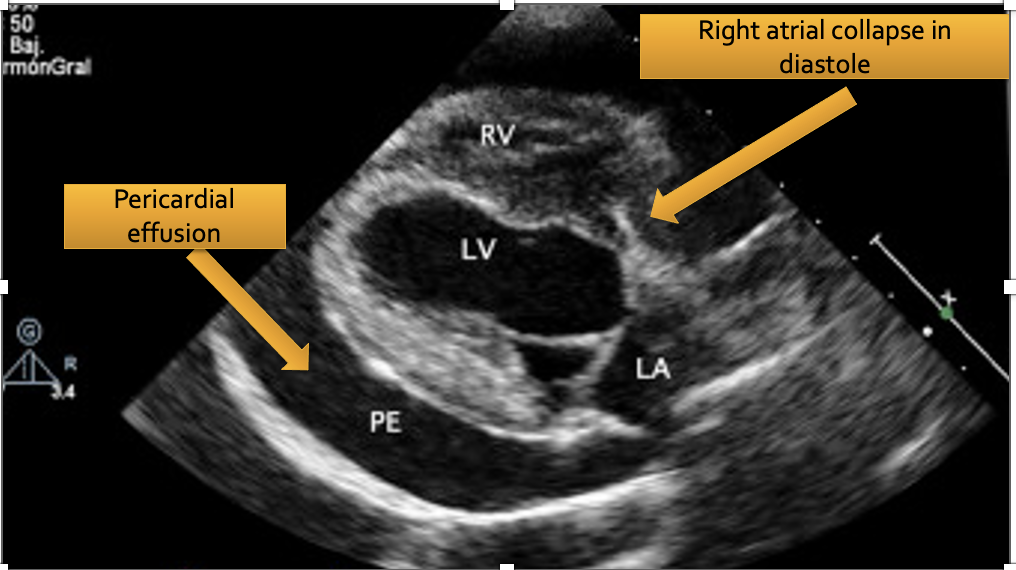
Figure 1. A right parasternal long axis view of the canine heart. This dog has cardiac tamponade physiology that is diagnosed based on the presence of shock and right atrial wall collapse in diastole.

Step 2: Assess left ventricle (LV) via right parasternal short/long axis and subxiphoid views using visual estimation of lumen size, gross wall contraction and wall thickening
Watch the video below:
- Hyperdynamic LV: A small LV lumen during systole and vigorous, hyperkinetic contractions obliterating the ventricle in systole (so-called “kissing” of the papillary muscles that come in contact during LV contraction);
- Hypodynamic LV: Minimal endocardial excursion towards the center of the LV; the interventricular septum and free LV wall don’t get thicker during contraction; there is an increased distance between the septal mitral leaflet and the interventricular septum at the end of diastole.
- Subjectively normal LV wall thickness, lumen size and contractility.
Watch the example of hypodynamic LV in a dog presenting with cardiogenic shock:
Step 3: Assess LA/Ao ratio in right parasternal short axis view
- Decreased LA/Ao: ratio objectively/subjectively smaller than 1.0; indicates (relative) hypovolemia or normal.
- Normal LA/Ao: ratio objectively/subjectively between 1.0 and 1.5; indicative of normovolemia or adequate preload.
- Increased LA/Ao: suggests cardiac disease causing increased left atrial volume and/or pressure or hypervolemia (ratio objectively greater than 1.5; subjectively enlarged)
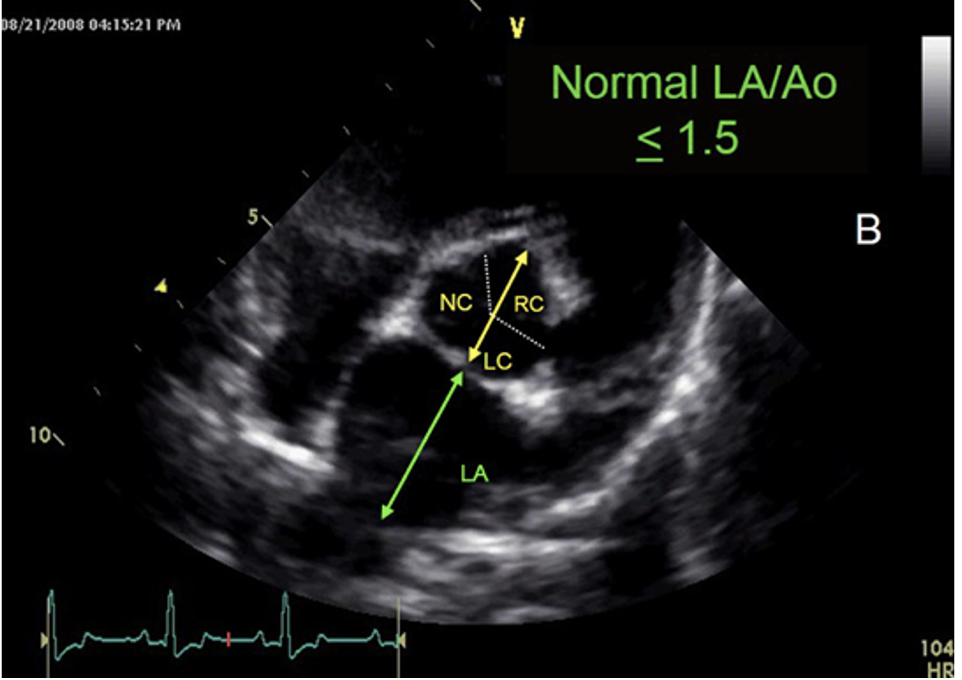
Figure 2. Normal left atrial to aortic diameter ratio (LA/Ao) in a dog.
Step 4: Assess the right ventricle (RV) via right parasternal short/long axis and subxiphoid views
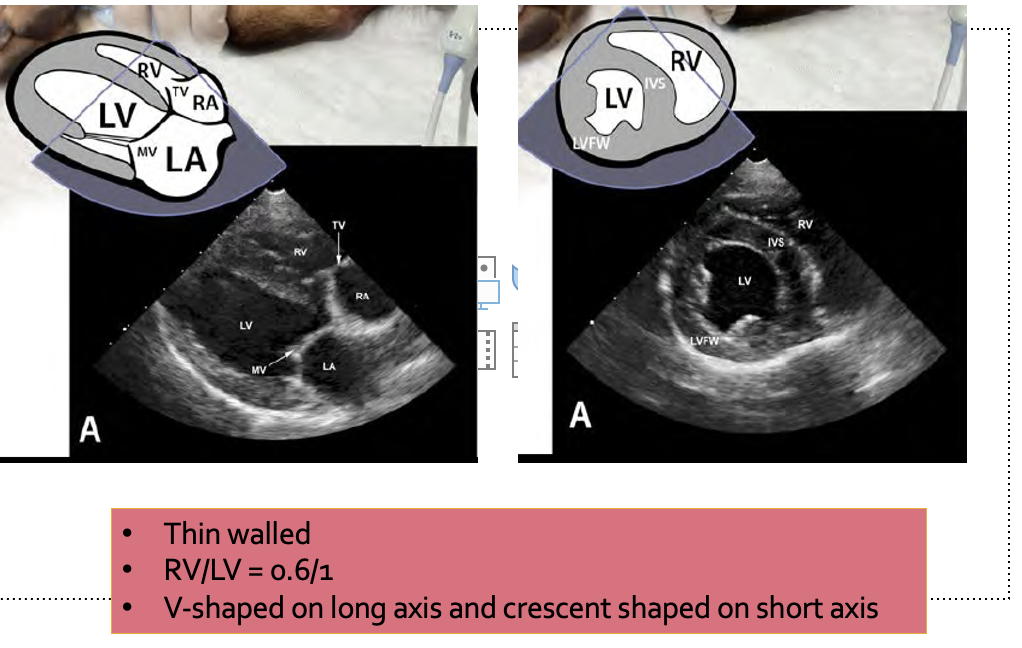
Figure 3. Assessment of the right ventricle with point-of-care ultrasound.
Right ventricular enlargement can be diagnosed if >2 or more listed below findings are present:
- RV > LV on right parasternal long and/or short axis view
- RA > LA on right parasternal long axis view
- Presence of interventricular septum (IVS) flattening (the interventricular septum will get deflected toward the LV lumen, causing a D shaped LV on right parasternal short axis view)
- Subjective free RV wall hypertrophy (thickness of the RV wall > free LV wall thickness)
Watch the example of severe RV enlargement in a canine patient who was presented in a right-sided congestive heart failure. He had severe pulmonary hypertension. His cage-side echo showed severe right-sided cardiomegaly:
Normal RV:
- On right parasternal short-axis view RV is smaller than LV, and it has a characteristic crescentic shape because it is wrapping around the circular shaped left ventricle;
- The RV walls are visibly thinner than left ventricular walls;
- On the right parasternal long-axis view, the RV has V shape. The RV to LV ratio is usually 0.4 to 0.6, in other words RV equal to 1/3-2/3 size of the LV.
CVC POCUS
The CVC is typically assessed via the subxiphoid view (B mode) (Darnis et al. 2017)
- The transducer is placed longitudinally under the subxiphoid process and angled cranially to visualize the diaphragm. The ultrasound probe then is fanned to the right of midline until the CVC could be identified at the point it crossed the diaphragm. The ultrasound probe then is slowly fanned off either side of the CVC and returned to the position where the CVC is subjectively felt to be at its widest diameter;
- The cineloop is assessed for the widest and narrowest diameter of the CVC on the abdominal side of the diaphragm during expiration and inspiration, respectively.
- The CVC diameter and its changes are subjectively assessed (see categories below);
CVC maximum diameter is subjectively assessed by an operator according to the categories listed below:
- Small CVC: Suggestive of (relative) hypovolemia, increased respiratory effort or increased intraabdominal pressure;
- Normal CVC: Suggestive of normovolemia.
- Increased CVC: Suggestive of elevated right atrial pressure
CVC Collapsibility Index (CVC CI) is determined by the following equation:
(CVCmax – CVCmin)/CVCmax x100% in B-Mode or M-Mode.
CVC collapsibility can be evaluated subjectively as well.
- CVC Collapsibility High: the subjective change in maximum and minimum CVC diameters is greater than 40-50%; indicative of a fluid responder, but can be also caused by increased respiratory effort and increased intra-abdominal pressure;
- CVC Collapsibility Normal: the subjective change in maximum and minimum CVC diameters is 25-35%; impossible to ascertain whether the patient would benefit from an additional fluid bolus.
- CVC Collapsibility Low: the subjective change in maximum and minimum CVC diameters is less than 25-30%; Indicative of an elevated right atrial pressure and likely represents a fluid-nonresponsive state
Below you can find an example of the canine CVC with increased diameter and minimal variation during respiratory cycle:
A insightful read from VETEMCRIT, highlighting the crucial role of point-of-care ultrasound (POCUS) in assessing intravascular volume status in emergency veterinary care. The integration of POCUS as a noninvasive diagnostic tool is a significant advancement, providing rapid and objective evaluation of physiologic parameters. The emphasis on its effectiveness, even when performed by non-cardiologists, speaks to the potential for enhancing diagnostic capabilities in emergency scenarios. Kudos to VETEMCRIT for promoting the importance of POCUS in veterinary medicine.