
Currently, veterinary emergency and critical care practitioners (diplomates, residents and emergency veterinarians) are divided into two camps: those that don’t use artificial colloids and those that do. Each camp has its own arguments in favor or against the use of synthetic colloids (hydroxyethyl starches, specifically). The objective of this blog post is NOT to convince the other party that he or she is wrong and I am right, but an attempt to find out what is true and what to do about it. The reader should understand that there will be a lot of personal opinions in this post, and, as always, I recommend to exercise your critical thinking before taking these statements for granted. Ray Dalio, one of the most successful investors of all times, called this process “thoughtful disagreement”, which is “the process of having a quality back-and-forth in an open minded and assertive way so as to see things through each other’s eyes. This is powerful because it helps both parties see things they’ve been blind to. It also helps to remind people that those who change their minds are the biggest winners because they learned something, whereas those who stubbornly refuse to see the truth are losers. With practice, training, and constant reinforcement, anyone can get good at this”.
Here are the most common arguments I have heard from my “pro-colloid” colleagues in favor of the use of hydroxyethyl starches (HESs):
- You need less volume of HES to resuscitate a hypovolemic patient;
- An HES bolus or CRI will increase colloid-osmotic pressure and, therefore, it will stay within the intravascular compartment for longer time, especially in patients with hypoalbuminemia and capillary leak syndrome (e.g. SIRS or sepsis);
- There is no high-quality evidence that HESs are harmful to veterinary patients;
If somebody wakes me up in the middle of the night and asks me why I personally never use HESs in my practice, I usually give them these 5 reasons:
- There is a fair number of studies in human medicine showing that HESs are harmful, especially in people with sepsis, acute kidney injury and critical illness; the evidence in veterinary medicine is not as robust, but molecular physiology of humans and canine/feline patients is very similar;
- There is no evidence that resuscitation with HESs vs. crystalloids is more beneficial or improves outcomes;
- The size of the HES molecules does not prevent them from being leaked out of the intravascular space in case of systemic inflammation or capillary leak;
- HESs are way more expensive than crystalloids;
- Why would I use a potentially harmful fluid without proven benefits that is also more expensive to my clients???
These are examples of different opinions in support or against the use of artificial colloids. As we know, opinions, even expressed by credible researchers and experts, possess the lowest level of evidence available to humankind. Let’s look at these opposing statements from the stand point of evidence-based medicine.
Argument #1: You need less volume of HES to resuscitate a hypovolemic patient.
According to Starling’s “three-compartment model,” crystalloids, with their sodium content similar to that of the serum, are distributed in the extracellular space (interstitial and intravascular), while colloids should remain intravascularly due to their large molecular weight. Therefore, theoretically four times more crystalloids should have the same volume expanding effect as colloids (Woodcock et al. 2012; László et al. 2017).
These relationships were proven in several experimental studies conducted on healthy animals. László et al. conducted an experiment where an anesthetized and mechanically ventilated pigs were randomized to receive a colloid (Voluven®, HES, n=15) or crystalloid (Ringerfundin®, RF, n=15) infusion. Animals were bled till baseline stroke volume index (SVI) dropped by 50% (T0), followed by resuscitation until initial SVI was reached (T4) in four steps. Invasive hemodynamic measurements, blood gas analyses and laboratory tests were performed at each assessment points. Glycocalyx degradation markers (Syndecan-1/hematocrit ratio, Glypican/hematocrit ratio) were determined at T0 and T4. Similar amounts of blood were shed in both groups (HES group: 506±159 mls blood, RF group: 470±127 mls blood). They found that animals received significantly less resuscitation fluid in the HES compared to the crystalloid group: 425 vs 1390 mls, p <0.001. The volume replacement ratio was 0.92 for HES; and 3.03 for the RF-group (p <0.001). There was no significant difference between the groups in the glycocalyx degradation markers.
Nevertheless, several clinical studies including thousands of critically ill people have seemingly disapproved the Starling principle, concluding that there were only marginal differences in the administered volume of crystalloid and colloid solutions – see Figure 1 (Annane et al. 2013; Guidet et al. 2012; Perner et al. 2012; Myburgh et al. 2012).
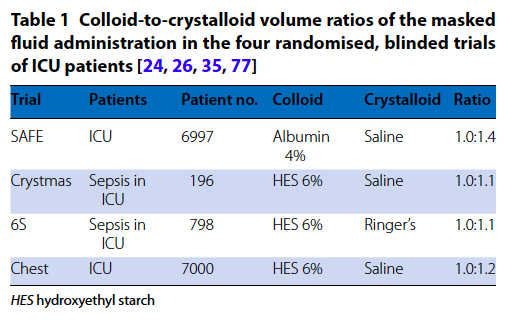
The Scandinavian trial (Perner et al. 2012) and CHEST trial (Myburgh et al. 2012) showed no significant difference in short-term hemodynamic resuscitation endpoints, apart from transient increases in central venous pressure and lower vasopressor requirements with HES in CHEST. The observed ratio of HES to crystalloid in these trials was approximately 1:1.3, which is consistent with the ratio of albumin to saline reported in the SAFE study (2004) and in other recent blinded, randomized, controlled trials of HES (James et al. 2011; Guidet et al. 2012).
These results might have been affected by the fact that most of the include patients were septic in whom the endothelial glycocalyx layer is often found to be impaired or destroyed, resulting in increased capillary permeability. Hence, colloids may disappear into the interstitial space in larger volumes than when the glycolcalyx is intact (Nelson et al. 2008; Chappell et al. 2009). Moreover, as reported in recent prospective studies (Johansson et al. 2011 and 2012), non-survivor trauma patients also had significantly higher circulating syndecan-1 concentrations than survivors, indicating an impairment in the endothelial glycocalyx (Nelson et al. 2008; Marechal et al. 2008). These results suggest that critical illness in general predisposes the patient to glycocalyx damage; hence, the volume-replacement ratio of crystalloids and colloids may be different from what would have been expected (László et al. 2017).
A recent comparative veterinary research study (Gauthier et al. JVECC 2014) evaluated the effect of tetrastarch administration on hemodynamic and laboratory variables in healthy dogs and dogs with lipopolysaccharide (LPS)-induced systemic inflammation, as compared with an equal volume of saline. Comparable volume-expanding efficacy was found after administration of saline or HES in both healthy and LPS-treated dogs. This was evidenced by similar changes in PCV and plasma protein concentration. Despite the provision of oncotic support, no significant beneficial effect on hemodynamic stabilization in the LPS-treated dogs was demonstrated with tetrastarch over normal saline. Dogs receiving tetrastarch had a significantly higher heart rate compared to dogs administered 0.9% NaCl, but there was no difference in RR, SBP or DBP between dogs administered 0.9% NaCl or tetrastarch (Gauthier et al. JVECC 2014).
My take-away is that the theoretical benefit of prolonged intravascular expansion by HESs does not hold true in every clinical scenario, especially in patients with impaired glycocalyx and systemic inflammation. This is the population of patients to whom artificial colloids are prescribed most commonly by “pro-colloid campers”.
Argument #2: HESs increase colloid-osmotic pressure and, therefore, will stay within the intravascular compartment for longer time, especially in patients with hypoalbuminemia and capillary leak syndrome (e.g. SIRS or sepsis) VS. The size of the HES molecules does not prevent them from being leaked out of the intravascular space in case of systemic inflammation or capillary leak.
HES solutions are produced by hydroxyethyl substitution of amylopectin obtained from sorghum, maize, or potatoes. A high degree of substitution on glucose molecules protects against hydrolysis by nonspecific amylases in the blood, thereby prolonging intravascular expansion, but this action increases the potential for HES to accumulate in reticuloendothelial tissues, such as skin (resulting in pruritus), liver, and kidney. Because of the potential that such solutions may accumulate in tissues, the recommended maximal daily dose of HES is 33 to 50 ml per kilogram of body weight per day.
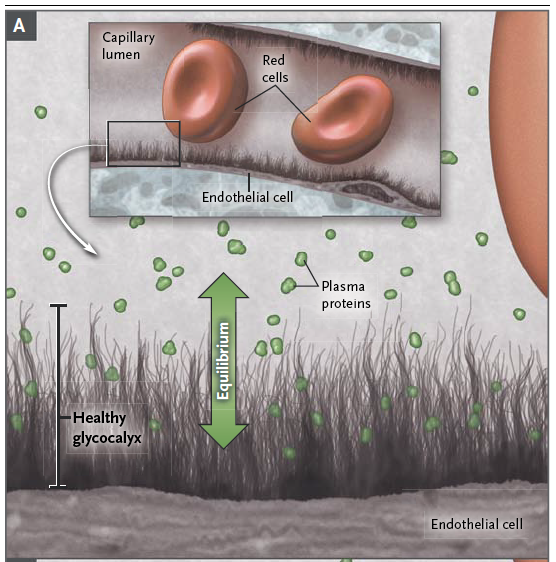
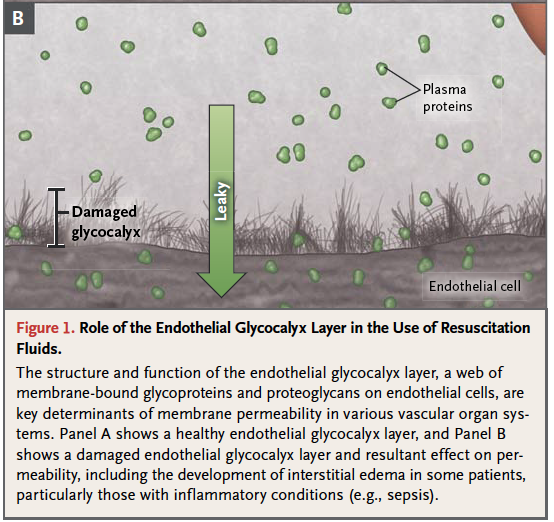
The structure and function of the endothelial glycocalyx (EG) layer are key determinants of membrane permeability in various vascular organ systems. The integrity, or “leakiness,” of this layer, and thereby the potential for the development of interstitial edema, varies substantially among organ systems, particularly under inflammatory conditions, such as sepsis, and after surgery or trauma, when resuscitation fluids are commonly used (Myburgh et al. 2013)- see Figures 2 and 3.
A recent excellent JVECC review article on EG (Gaudette et al.) described a study where isolated guinea pig hearts were used to measure fluid extravasation after perfusion with either albumin or HES. Although HES led to a higher COP compared to albumin, it did not reduce the capillary permeability to the same extent that albumin did. These findings suggest that different colloids have different effects on transvascular fluid flux and that the ability of albumin to afford reduced vascular permeability could be due at least partially to its incorporation into the EG (Jacob et al, 2007). Gaudette et al. stated that, “albumin appears to be able to penetrate and bind within the EG thereby reforming the endothelial surface layer (ESL) and restoring vascular integrity. In comparison, HES only partially improved the ESL barrier, being superior to crystalloids alone but inferior to albumin (Jacob et al. 2006)”.
Conversely, in a randomized controlled trial of people undergoing coronary artery bypass graft placement, “the administration of HES was associated with increased EG degradation, as measured by plasma SDC1 concentrations, compared to the use of crystalloids (Kim et al. 2017). The balance of evidence suggests that synthetic colloids are not superior to crystalloids for the preservation of the EG, calling into question the clinical utility of HES. It is possible that providing albumin to reconstitute the EG in critical illness could help restore microvascular barrier function, but the appropriate albumin dose to achieve a beneficial effect remains unknown”.
Colloids’ half-life and efficacy during systemic inflammatory conditions are probably reduced because of an increase in capillary permeability (Vercueil et al. 2005), although other studies point on the opposite way. Marx et al. (2002) compared the effects of Ringer solution (RS), gelatin, and HES 200/0.5 on a porcine model of septic shock, with fluids titrated to a central venous pressure of 12 mmHg. Colloids were more effective on keeping plasma volume stable than RS. However, no difference between the colloids was noted regarding capillary leak as measured by albumin escape rate.
My take-away is that, taken together, experimental studies suggest that when a fluid challenge is performed aiming to increase cardiac output on preload responsive patients, a smaller amount of colloids is equally effective as a larger amount of crystalloids. Colloids do preserve plasma oncotic pressure, but nobody knows if that is beneficial. The efficacy of colloids appears to be preserved in some studies on patients with experimental sepsis, although it remains uncertain if they have any positive effect on capillary leak and it is not proven in clinical human trials.
Argument #3: There is no high-quality evidence that HESs are harmful to veterinary patients
Despite the recent surge in clinical data in the field of human critical care, minimal safety and efficacy data exist in veterinary medicine regarding the use of HES as a resuscitation fluid. The large-scale veterinary clinical trials required to establish an influence of HES resuscitation on patient outcome and adverse effects are likely not logistically feasible in the near future (Cazzolli et al 2015). As always, caution must be used when extrapolating human data and associated conclusions to veterinary patient populations given several patient and population-dependent factors, which confer an inherent risk of error.
A few veterinary retrospective studies showed inconsistent results in regards to the safety of HES in dogs.
Hayes et al. (JVECC 2015) published a retrospective cohort study on the incidence of acute kidney injury and death following hydroxyethyl starch (HES 10% 250/0.5/5:1) administration in dogs (2007–2010). The primary outcome was a composite of in‐hospital death or AKI. In an adjusted analysis after controlling for illness severity, admission type, and concurrent administration of blood products, HES administration remained an independent risk factor for the composite adverse outcome (OR = 1.98, P = 0.005), with a number needed to harm (NNH) = 6.
Yozova et al. (JVECC 2016) performed a retrospective evaluation of the effects of administration of tetrastarch (hydroxyethyl starch 130/0.4) on plasma creatinine concentration in dogs. Two hundred and one dogs admitted to the intensive care unit with initial plasma creatinine concentrations not exceeding laboratory reference intervals and receiving either crystalloids alone (CRYS group, n = 115) or HES with or without crystalloids (HES group, n = 86) for at least 24 hours. HES administration in this canine population did not result in increased creatinine concentrations compared to administration of crystalloids. Further studies are needed to establish the safety of HES in critically ill dogs.
Boyd et al. (JVECC 2019) evaluated biomarkers of kidney injury following 4% succinylated gelatin and 6% hydroxyethyl starch 130/0.4 administration in a canine hemorrhagic shock model. In dogs with hemorrhagic shock, gelatin was associated with greater magnitude increases in urine biomarkers of AKI and more frequent marked tubular microvesiculation, compared with fresh whole blood, crystalloids, and HES.
Argument #4 (against HESs): There is a fair number of studies in human medicine showing that HES are harmful, especially in people with sepsis, acute kidney injury and critical illness; the evidence in veterinary medicine is not as robust, but molecular physiology of humans and canine/feline patients is very similar.
The last iteration of the Surviving Sepsis Campaign states that, “We recommend against using hydroxyethyl starches (HESs) for intravascular volume replacement in patients with sepsis or septic shock (strong recommendation, high quality of evidence). Overall, the undesirable consequences of using HES (increased risk of death and need for RRT) along with moderate to high quality of available evidence resulted in a strong recommendation against the use of HES in resuscitation of patients with sepsis or septic shock.”
A meta-analysis of nine trials (3,456 patients) comparing 6% HES 130/0.38–0.45 solutions to crystalloids or albumin in patients with sepsis showed no difference in all-cause mortality (Haase 2013). However, when low risk of bias trials were analyzed separately, HES use resulted in higher risk of death compared to other fluids (RR, 1.11; high-quality evidence), which translates to 34 more deaths per 1,000 patients. Furthermore, HES use led to a higher risk of renal replacement therapy, RRT (RR, 1.36; high-quality evidence) (Haase 2013).
A subsequent network meta-analysis focused on acute resuscitation of patients with sepsis or septic shock and found that HES resulted in higher risk of death (10 RCTs; OR, 1.13; high-quality evidence) and need for RRT (7 RCTs; OR, 1.39; high-quality evidence) compared to crystalloids.
When comparing albumin to HES, albumin resulted in lower risk of death (OR, 0.73; moderate-quality evidence) and a trend toward less need for RRT (OR, 0.74; low quality evidence) (Rochwerg et al. 2014).
In a blinded, randomized, controlled trial involving 800 patients with severe sepsis in the ICU (Perner et al. 2012), Scandinavian investigators reported that the use of 6% HES (130/0.42), as compared with Ringer’s acetate, was associated with a significant increase in the rate of death at 90 days (relative risk, 1.17; P = 0.03) and a significant 35% relative increase in the rate of renal-replacement therapy. These results are consistent with previous trials of 10% HES (200/0.5) in similar patient populations (Brunkhorst et al. 2008).
What about evidence on the use of HES in the general population of patients with various causes of critical illness?
In 2012, the results of the Crystalloid versus Hydroxyethyl Starch Trial (CHEST) were published (Myburgh et al. 2012). CHEST was a randomized, controlled trial in which 6% hydroxyethyl starch with a molecular weight of 130 kD and a molar substitution ratio of 0.4 (130/0.4, Voluven) in 0.9% sodium chloride was compared with 0.9% sodium chloride (saline) for fluid resuscitation in critically ill patients with various disorders, including trauma, sepsis, and post-operative patients (a total of 7000 people). The trial showed no significant difference in the primary outcome (mortality at 90 days) between the hydroxyethyl starch and saline groups, but it showed that hydroxyethyl starch was associated with a significant increase in the use of renal replacement therapy. These and other data (Mutter et al. 2013) led medical regulatory authorities to amend licensing and restrict the use of hydroxyethyl starch in specific patient populations.
Argument #5 (against HESs): There is no evidence that resuscitation with HES or other colloids vs. crystalloids is more beneficial or improves outcomes.
“The absence of a confirmed survival advantage in conjunction with increased documentation of adverse effects is the core of the controversy of continued use of colloidal solutions in the resuscitation of critically ill human patients”
Cazzolli et al. 2015
A recent Cochrane review (Lewis et al. 2018) looked at the available evidence comparing colloids with crystalloids in critically ill people. They identified 69 relevant studies with 30,020 critically ill participants who were given fluid replacement in hospital or in an emergency out-of-hospital setting. They found moderate-certainty evidence that using colloids (starches; dextrans; or albumin or FFP) compared to crystalloids for fluid replacement probably makes little or no difference to the number of critically ill people who die within 30 or 90 days, or by the end of study follow-up. They also found moderate-certainty evidence that using starches probably slightly increases the need for blood transfusion. However, they were uncertain whether using other types of colloids, compared to crystalloids, makes a difference to whether people need a blood transfusionbecause the certainty of the evidence is very low. Another findings with moderate-certainty evidence was that using starches for fluid replacement probably slightly increases the need for renal replacement therapy.
Argument #6 (against HESs): HESs are way more expensive than crystalloids.
The math is very simple. The cost of a 500 ml Vetstarch bag is $45. The cost of a 1000 ml LRS bag is $7 (U.S. costs).
The Bottom Line
The only fact is that the use of synthetic colloids in veterinary medicine is going to remain one of the most controversial topics of all times. There are experimental studies conducted on healthy and sick animals showing benefits of colloids, however there are studies showing the opposite results. There is compelling evidence supporting avoidance of use of HES solutions in certain human patient populations, including patients with known renal dysfunction and patients with sepsis, systemic inflammation or suspected severe capillary leak and third spacing. To the best of my knowledge, there are literally no high-quality prospective veterinary studies that would attempt to investigate the safety or efficacy of HES vs. crystalloids in a clinical setting. Unfortunately, this type of studies may never be performed due to various economical and organizational aspects.
At this point in time, the decision to use or not to use synthetic colloids becomes a personal decision that every emergency and critical care practitioner has to make. I made this decision about 4-5 years ago. I don’t want to use a fluid solution that may cause potential harm (not proven in clinical veterinary patients, but proven in people), and has questionable benefits that were shown only in some experimental settings. In my humble opinion, HESs’ potential harm + their questionable benefits are worse than crystalloids’ relative safety (if judiciously used) + non-inferiority.
The way I prefer to resuscitate hemodynamically unstable patients with high fluid requirements, capillary leak and wide-spread edema is crystalloids + very early administration of low-dose norepinephrine that will recruit non-stressed volume pooled in venous compartment without causing arterial vasoconstriction. One of the next blog posts will be dedicated to this extremely interesting topic. Hypoalbuminemia should be treated by early enteral nutrition and by addressing an underlying disease instead of administration of artificial substances that accumulate in the body tissues for years.
References
- László et al. Volume-replacement ratio for crystalloids and colloids during bleeding and resuscitation: an animal experiment. Intensive Care Medicine Experimental, 2017.
- Woodcock et al. Revised Starling equation and the glycocalyx model of transvascular fluid exchange: an improved paradigm for prescribing intravenous fluid therapy. Br J Anaesth 2012.
- Haase et al. Hydroxyethyl starch 130/0.38- 0.45 versus crystalloid or albumin in patients with sepsis: systematic review with meta-analysis and trial sequential analysis. BMJ 2013.
- Rochwerg et al. Fluids in Sepsis and Septic Shock Group: Fluid resuscitation in sepsis: a systematic review and network meta-analysis. Ann Intern Med 2014.
- Vercueil et al. Physiology, pharmacology, and rationale for colloid administration for the maintenance of effective hemodynamic stability in critically ill patients. Transfus Med Rev, 2005.
- Marx et al. Hydroxyethyl starch and modified fluid gelatin maintain plasma volume in a porcine model of septic shock with capillary leakage. Intensive Care Med, 2002.
- Myburgh et al. Resuscitation Fluids. CCM 2013.
- Jacob et al. The endothelial glycocalyx affords compatibility of Starling’s principle and high cardiac interstitial albumin levels. Cardiovasc Res. 2007.
- Myburgh et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N Engl J Med 2012.
- Mutter et al. Hydroxyethyl starch (HES) versus other fluid therapies: effects on kidney function. Cochrane Database Syst Rev 2013.
- Lewis et al. Colloids versus crystalloids for fluid resuscitation in critically ill people. Cochrane Database of Systematic Reviews 2018.
- Perner et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med 2012.
- Brunkhorst et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008.
- The SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004.
- James et al. Resuscitation with hydroxyethyl starch improves renal function and lactate clearance in penetrating trauma in a randomized controlled study: the FIRST trial (Fluids in Resuscitation of Severe Trauma). Br J Anaesth 2011.
- Guidet et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: the CRYSTMAS study. Crit Care 2012.
- Annane et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock. JAMA 2013.
- Finfer et al. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004.
- Nelson et al. Increased levels of glycosaminoglycans during septic shock: relation to mortality and the antibacterial actions of plasma. Shock 2008.
- Chappell et al. The impact of the glycocalyx on microcirculatory oxygen distribution in critical illness. Curr Opin Anaesthesiol 2009.
- Johansson et al. Elderly trauma patients have high circulating noradrenaline levels but attenuated release of adrenaline, platelets, and leukocytes in response to increasing injury severity. Ann Surg 2011.
- Johansson et al. High circulating adrenaline levels at admission predict increased mortality after trauma. J Trauma Acute Care Surg 2012.
- Nelson et al. Increased levels of glycosaminoglycans during septic shock: relation to mortality and the antibacterial actions of plasma. Shock 2008.
- Marechal et al. Endothelial glycocalyx damage during endotoxemia coincides with microcirculatory dysfunction and vascular oxidative stress. Shock 2008.
- Cazzolli et al. The crystalloid-colloid debate: Consequences of resuscitation fluid selection in veterinary critical care. JVECC 2015.
- Gauthier et al. Effect of synthetic colloid administration on hemodynamic and laboratory variables in healthy dogs and dogs with systemic inflammation. JVECC 2014.
- Zersen et al. Retrospective evaluation of paired plasma creatinine and chloride concentrations following hetastarch administration in anesthetized dogs (2002–2015): 244 cases. JVECC 2019.
- Gaudette et al. The endothelial glycocalyx: Structure and function in health and critical illness. JVECC 2020.
- Jacob et al. Contrasting effects of colloid and crystalloid resuscitation fluids on cardiac vascular permeability. Anesthesiology 2006.
- Kim et al. Microvascular reactivity and endothelial glycocalyx degradation when administering hydroxyethyl starch or crystalloid during off‐pump coronary artery bypass graft surgery: a randomised trial. Anaesthesia 2017.