
This blog outlines a practical, evidence-based approach to deciding when treatment for Enterococcus in septic peritonitis is truly warranted in dogs and cats.
A 7-year-old spayed female Persian cat was presented to an emergency service for evaluation of fever, chronic vomiting, and severe lethargy. On initial examination, the cat was stuporous, with fair femoral pulses, pale pink mucous membranes, moderate dehydration, a body temperature of 104°F (40°C), and a heart rate of 150 beats per minute.
The initial work-up suggested septic peritonitis and partial jejunal mechanical obstruction, based on abdominal ultrasound and abdominal fluid cytology. Stabilization included fluid resuscitation and intravenous antibiotics (ampicillin/sulbactam at 30 mg/kg IV q8h and enrofloxacin at 5 mg/kg IV q24h), followed by norepinephrine (0.1 mcg/kg/min) due to persistent arterial hypotension.
Three hours after presentation, the cat underwent exploratory laparotomy, which revealed a foreign body in the jejunum causing obstruction and perforation. Post-lavage peritoneal swabs were submitted for culture and sensitivity. The cat received resection and anastomosis, along with JP drain placement. Norepinephrine was discontinued 36 hours post-surgery, and nasogastric tube feeding was initiated shortly thereafter.
Culture and sensitivity results showed the following growth within 2-3 days:
- Candida albicans: A commensal fungal organism normally present in low numbers in the gastrointestinal, oral, and urogenital tracts of cats. However, it can cause peritonitis when it enters the peritoneal cavity, often due to gastrointestinal perforation or surgery-related contamination.
- Bacteroides stercoris: It is a species of anaerobic, Gram-negative bacteria commonly found in the human and animal gastrointestinal tract. Although it is part of the normal gut flora, Bacteroides stercoris can become pathogenic if it enters parts of the body where it doesn’t belong, such as the peritoneal cavity. This can occur in cases of gastrointestinal perforation or abdominal trauma, leading to septic peritonitis.
- Enterococcus faecium (see sensitivity results in Figure 1; enterococcus in septic peritonitis).
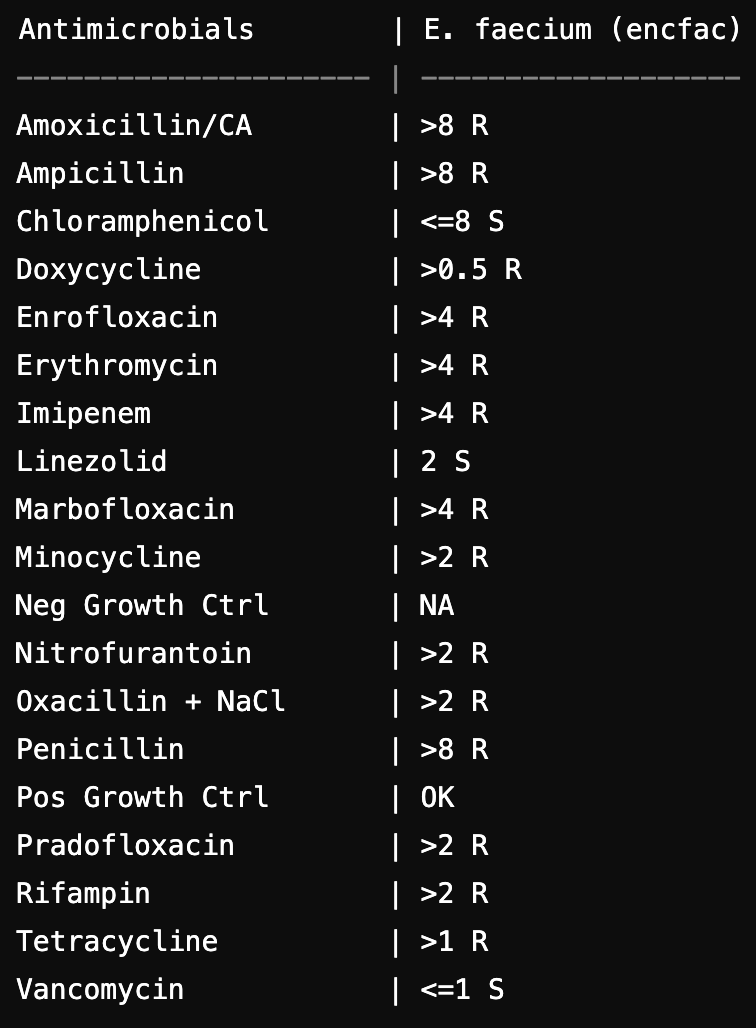
Figure 1. Antibiotic sensitivity of E. faecium cultured from peritoneal effusion in the cat with septic peritonitis. “R” stands for “Resistant”; “S” stands for “Sensitive”; “NA” stands for “Not Applicable”.
In this blog article, we will focus on the enterococcus in septic peritonitis in dogs and cats. Enterococci are commensal bacteria inhabiting GI tract of animals and humans. It typically emerges in debilitated patients exposed to broad-spectrum antibiotics and as part of polymicrobial infections (especially, GI and/or urogenital). Enterococci are usually part of mixed aerobic and anaerobic flora, and antimicrobial regimens with minimal in vitro anti-enterococcal activity are often effective in treating mixed infections; therefore, the pathogenicity of enterococci in this setting is questionable. These and other factors limit the ability of investigators to determine the independent contribution of enterococcal infections to mortality and morbidity.

It is not uncommon to see a positive enteroccocal growth in patients with septic abdomen. Unfortunately, these bacteria commonly possess inherited and acquired resistance to multiple classes of antibiotics (multidrug resistant, MDR).
For example, E. faecium has inherited resistance to penicillinase-susceptible penicillin (low level), penicillinase-resistant penicillins, cephalosporins, nalidixic acid, aztreonam, macrolides, and low levels of clindamycin and aminoglycosides (Fraser et al. 2018). It commonly acquires resistance to chloramphenicol, tetracyclines, rifampin, fluoroquinolones, aminoglycosides (high levels), and even vancomycin (Vancomycin Resistant Enterococcus, VRE).
Aminopenicillins arrest their growth but do not kill the bacteria; Enterococci promptly produce B-lactamases after exposure to the beta–lactamase inhibitors. The combination of aminoglycosides or ceftriaxone and aminopenicillins may be used to enhance their individual effects (Fernández-Hidalgo et al. 2013) against E.faecalis but not E.faecium. Besides vancomycin and beta-lactam/aminoglycoside combination, enterococci may be sensitive to doxycycline, rifampin and chloramphenicol.
In my clinical practice, it is very common when a dog or cat receives a definitive surgical treatment for a septic abdomen, starts to improve in the first 2-3 days after surgery, and the initial abdominal fluid culture comes back positive for Enterococci in combination with E.coli or other polymicrobial flora. E.faecium is usually MDR and chloramphenicol or rifampin are only antibiotics that this bacterium is sensitive to on the standard culture/sensitivity report (whereas an extended report may include sensitivity to the antibiotics of last resort such as linezolid and vancomycin).
The question arises: should we ignore the growth of Enterococcus in septic peritonitis case, given the patient is improving and its virulence has been debated in both human and veterinary literature, or should we treat this bacterium? To address this, I created a guideline after reviewing the relevant human and veterinary literature.
The guideline can be used in all patients with a positive culture growing Enterococcus spp (most common in septic abdomen secondary to GI perforation, wounds, and urogenital infections). Since the Enterococcus spp. (especially, E. faecium) has an extensive inherited and acquired antibiotic resistance and the virulence of this bacterium is controversial and not always implicated in a syndrome of sepsis, the treatment of positive Enterococcal cultures is not always warranted.
Step 1: Determine the risk of not treating Enterococcus.
Low risk patients
- Hemodynamically stable
- No new organ dysfunctions
- Immunocompetent, not receiving immunosuppressive therapy
High risk patients
- Patients with septic shock
- Worsening clinical status, development of a new organ dysfunction
- Immunocompromised patients (neutropenic, undergoing chemotherapy, receiving immunosuppressive drugs)
- Patients with persistent intra-abdominal fluid collections without clinical improvement and in whom definitive source control cannot be achieved;
- Patients with suspected bacterial endocarditis
Step 2: If the patient is considered a low risk for developing complications secondary to Enterococcus infection and the source control is achieved (e.g. an abscess is drained, septic abdomen is corrected, etc), you may consider:
- Not treat Enterococcus + treat other bacteria (in case of polymicrobial culture results) + continue monitoring the patient; if the patient becomes a high risk, it is recommended to consider starting antibiotic therapy specific for Enterococcus;
- Perform a blood culture from at least 2 different veins; if the culture is negative and the patient remains a low risk, do not treat Enterococcus; if the Enterococcal bacteremia is confirmed on the blood culture, start anti-enterococcal therapy (Step 3) (Claeys et al. 2016).
Step 3: In general, if the patient is a high risk (see Step 1) and has a positive Enterococcal growth, the treatment of this infection is likely warranted (Chatterjee et al 2007).
- Start the specific anti-enterococcal therapy once the culture/sensitivity results are back
- Choose the antibiotic with the least toxic potential (most common antibiotics that E.faecium remains sensitive to include doxycycline, chloramphenicol and rifampin)
- If E.faecium is resistant to mentioned-above antibiotics and the patient remains a high risk, vancomycin can be considered as a last resort option, however the antibiotic use committee should be consulted prior to its use. Vancomycin-resistant Enterococcus (VRE) is an emergent pathogen that is becoming more prevalent in human medicine.
The cat described at the beginning of this article was initially started on fluconazole (for Candida spp.), metronidazole (based on Bacteroides sensitivity), and chloramphenicol for E. faecium. However, chloramphenicol was discontinued shortly after, as the cat’s blood cultures returned negative and its cardiovascular status had normalized.
The Bottom Line
Reflecting on this case, Enterococcus was isolated as part of a polymicrobial infection in a patient who showed signs of improvement after surgical intervention. Although it’s tempting to act on any positive culture result, we must carefully weigh the patient’s overall status and the potential risks of treatment. In stable, low-risk patients, withholding anti-enterococcal therapy might be a safe option, but this decision should never be made lightly. Blood cultures can offer additional guidance, but clinical judgment remains paramount. For those in more critical states, we must be cautious with antibiotic selection, always considering the potential for resistance while avoiding unnecessary exposure to last-resort antibiotics.
MASTER MANAGEMENT OF ELECTROLYTE AND ACID-BASE DISORDERS
WITH THE MOST EFFECTIVE RACE-APPROVED ONLINE TRAINING PROGRAM
References
Arias CA, Murray BE. The rise of the Enterococcus: beyond vancomycin resistance Nat Rev Microbiol. 2012;10:266–278
Hardie JM, Whiley RA. Classification and overview of the genera Streptococcus and Enterococcus. J Appl Microbiol. 1997;83:1S–11S
de Perio MA, Yarnold PR, Warren J, et al. Risk factors and outcomes associated with non-Enterococcus faecalis, non-Enterococcus faecium enterococcal bacteremia. Infect Control Hosp Epidemiol. 2006 Jan. 27(1):28-33
Chatterjee I, Iredell JR, Woods M, et al. The implications of enterococci for the intensive care unit. Crit Care Resusc. 2007 Mar. 9(1):69-75
Claeys KC, Zasowski EJ, Lagnf AM, Rybak MJ. Comparison of outcomes between patients with single versus multiple positive blood cultures for Enterococcus: Infection versus illusion?. Am J Infect Control. 2016 Jan 1. 44 (1):47-9
Fernández-Hidalgo N, Almirante B, Gavaldà J, Gurgui M, Peña C, de Alarcón A, et al. Ampicillin plus ceftriaxone is as effective as ampicillin plus gentamicin for treating enterococcus faecalis infective endocarditis. Clin Infect Dis. 2013 May. 56(9):1261-8
Susan L Fraser, MD et al. Enterococcal Infections Treatment & Management. Medscape 2018.
Great post! I think that another article to consider which supports the confusion regarding this issue and the general idea that if the source of contamination is addressed, antibiotic selection may be less important is Kalafut JAAHA 2018 Comparison of Initial and Postlavage Bacterial Culture Results of Septic Peritonitis in Dogs and Cats”
“Positive culture pre- or postlavage and appropriate antimicrobial selection did not significantly affect survival. For individual animals, culture results differed between pre- and postlavage samples, although no definitive effect of peritoneal lavage was seen for the population as a whole. Antimicrobials most commonly effective against isolates were Cefotaxime, Ceftazidime, and Imipenem. If prompt surgical source control is employed, antibiotic choice may not affect clinical outcome.”
It can be really frustrating if the patient is not improving clinically and then deciding to reach for a “big gun” versus waiting for blood culture results..no easy answers! I would also say that progression of cytology of the abdominal fluid can be helpful while waiting for other diagnostics.
Great thoughts, Cleo. I appreciate your input!
Even though that the analysis may show sensitivity to a certain antimicrobial medicines in vivo, enterococcus can still be resistant to them in vitro. This is super bacteria that can over-live us all and can grow in acetic environment, in the presence of high salt concentration and survives prolonged fasting. Therefore, some sort of special approach should be used to treat the bacteria. Certainly, only pathogen strains should be treated.